Two successful candidates in the CGDent and GC Award for Foundation Trainees 2024/25, Dental Therapist Ruba Al-Nuaimy and Dentist Karan Ahir, describe taking part in the competition and what they gained from the experience.

Q. What’s your dental role and which DFT Region are you in?
Ruba Al-Nuaimy: I am a Dental Therapist and Hygienist on the North West scheme.
Karan Ahir: I am a Foundation Dentist in the West Yorkshire Scheme.
Q. Why did you decide to enter the CGDent-GC Award?
RA: I entered the competition because it was a great opportunity to showcase my clinical skills and challenge myself early in my career. When I saw that this was the first year the award was open to Dental Therapists, I knew I had to try, as it felt like the perfect way to step outside my comfort zone.
I’ve always been motivated by pushing myself to grow, and this felt like a chance to take my work to the next level. It was exciting to present a case that tested both my technical ability and creativity, while also highlighting the important role dental therapists can play in delivering high-quality patient care. Entering has been a hugely rewarding experience, and I see it as an important step in building my confidence and continuing to develop as a clinician.
KA: I genuinely enjoy the challenge and artistry involved in placing anterior composites, which is why I decided to enter. Restoring both function and aesthetics in such a visible area is highly rewarding, and I was keen to showcase the work I have carried out in this case.
Also having the opportunity to attend a renowned anterior composite course particularly excited me, as it offered an opportunity to further refine my skills, learn advanced techniques, and ultimately deliver even higher quality outcomes for my patients. I saw this competition not only as a platform to share my work but also as a valuable step in my professional development, enabling me to continually improve and grow as a clinician.
Q: Can you describe the case you entered?
RA: A 26-year-old male patient with Autism and learning difficulties was referred by his GDP. He presented with poor oral hygiene, generalised gingivitis, and multiple anterior carious lesions. His main concerns were painful, bleeding gums and the dark cavities visible when smiling, which were affecting both comfort and confidence.
I implemented a phased treatment plan with the initial focus on stabilising active gingival disease through behaviour management, tailored oral hygiene instruction, and non-surgical periodontal therapy including supra- and subgingival scaling. Once periodontal health improved, I proceeded with restoring the anterior teeth using direct composite restorations under rubber dam isolation, adopting a minimally invasive approach to preserve tooth structure and restore aesthetics.
This case was particularly rewarding as it challenged me to adapt my communication style and treatment planning to suit the patient’s additional needs. By using clear, jargon-free explanations, visual aids, and goal setting, I was able to improve his daily oral care engagement and achieve a functional and aesthetic outcome that met his expectations.


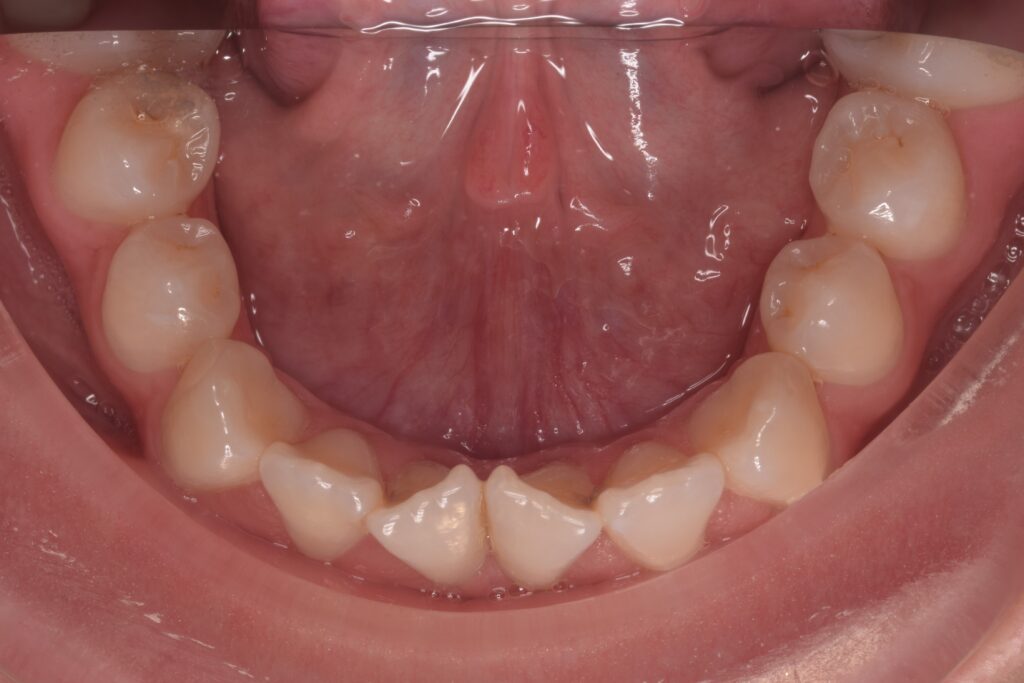
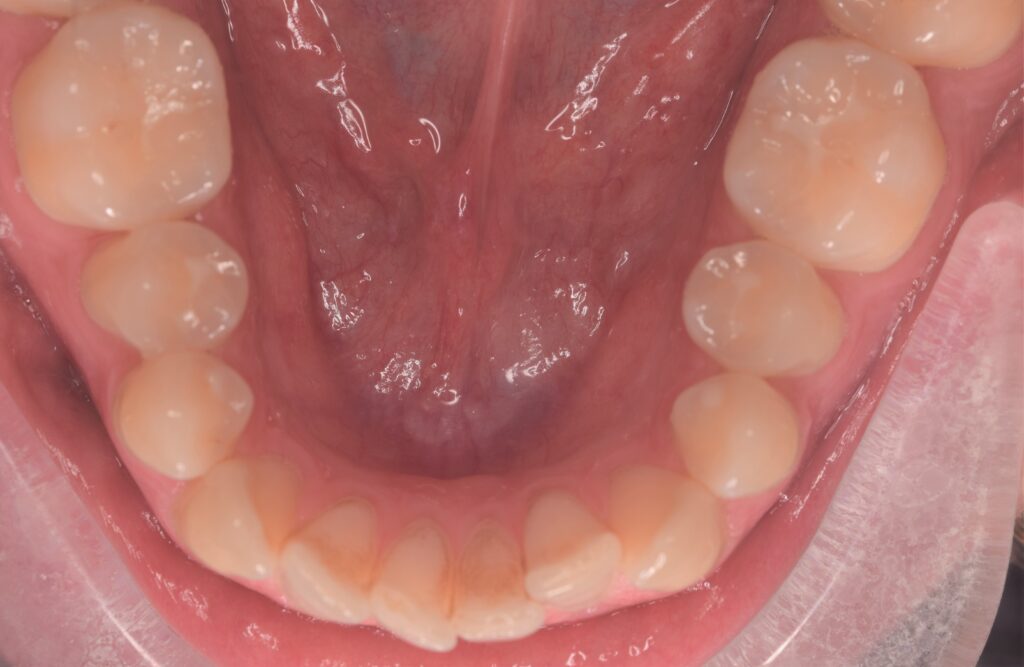
KA: A 40-year-old fit and well female presented with missing posterior teeth and failing anterior restorations, beneath which was severe anterior tooth surface loss (TSL), causing functional difficulty and dissatisfaction with her appearance. The aetiology was multifactorial: past unstable GORD, high intake of fizzy drinks, and nocturnal bruxism. Posterior teeth had previously been extracted due to erosion and caries, though the patient remained periodontally stable. She declined NHS referral after being previously refused treatment, so care was undertaken locally.
Treatment provided included OHI, preventive advice, and initial composite restorations. A diagnostic wax-up was used to guide upper anterior composite build-ups at an increased OVD, completed with a palatal stent and freehand layering. A soft lower occlusal splint was provided for protection, and Co-Cr upper and lower partial dentures were fitted to restore posterior support and reduce anterior load. The patient adapted well, expressed satisfaction with both function and appearance, and was motivated to maintain reduced fizzy drink intake and attend for ongoing reviews.



Q. How will you adapt your practice as a result of attending the composite layering course?
RA: Attending the composite layering course has really changed the way I approach restorative work. I feel more confident with freehand composite placement, particularly in shade selection, anatomical build-up, and creating natural depth in restorations. We also learnt about a wide range of materials and their indications, such as using injectable composite for stamp technique posterior restorations, as well as the importance of choosing dentine and enamel shades appropriately.

The course also highlighted how crucial it is to understand light perception and refraction in order to achieve lifelike results. Since then, I’ve been more deliberate in how I replicate translucency and natural contours, which has helped me deliver more seamless and aesthetic outcomes.
I’ve refined my finishing and polishing routine too, aiming for smooth contours and a high-gloss finish that improves both aesthetics and longevity. Overall, the course has given me the confidence to take on more challenging anterior cases and motivated me to keep developing my skills so I can deliver predictable results that are both functional and highly aesthetic.
KA: After attending the composite layering course, I want to apply what I’ve learned to make my anterior restorations look as natural as possible. By using advanced layering techniques, I can better replicate the optical properties of enamel and dentine, creating restorations that blend seamlessly with surrounding teeth while remaining durable and functional.

I also feel more confident in using opaquers for discoloured cases. Now that I understand the correct technique and application, I will incorporate them more often. This will allow me to mask underlying discolouration effectively without relying on excessive dentine composite, resulting in restorations that are both more aesthetic and less bulky.
In addition, I will refine my finishing and polishing by following the protocols demonstrated during the course. This will help me achieve a higher-quality surface finish, enabling restorations to maintain their shine and resist staining for longer, outcomes that patients will both notice and value.
Q. Has your success in the CGDent-GC Award impacted you in any other ways?
RA: Winning the Award has hugely boosted my confidence and reinforced my passion for dentistry. Being the only Dental Therapist to receive the award made it especially meaningful, as it highlighted the importance of our role and the ever-expanding scope of practice available to us. It reminded me that I am not limited to certain treatments, and that with the right training and mindset, therapists can take on complex, rewarding cases. It has also encouraged me to seek further opportunities, step outside my comfort zone, and keep building on my skills with greater confidence. I hope this achievement motivates other Dental Therapists to recognise their potential and embrace the opportunities our profession offers to make a real difference for patients, while striving to provide the highest standard of care.

KA: Being successful in the CGDent-GC Award has significantly increased my confidence in anterior composite work and motivated me to continue developing my restorative skills. It has inspired me to attend further restorative courses to broaden my knowledge and stay up to date with best practices. I also aim to share the techniques and insights I’ve gained with colleagues, helping to raise standards within my team. Beyond technical skills, the award has reminded me of the profound impact well-executed restorative work can have on patients’ confidence and quality of life.

Q. What would you say to other Foundation Trainees thinking of entering the Award?
RA: I would strongly encourage Foundation Trainees to enter the Award, particularly Dental Therapists. It’s an incredible opportunity to showcase your abilities, gain recognition early in your career, and demonstrate the valuable role therapists play within dentistry. For me, one of the most rewarding aspects was meeting other trainees, sharing experiences, and realising how much we can learn from one another. I gained valuable perspective from dentists, and in turn they learnt more about the scope and contribution of Dental Therapists, which made it a really collaborative experience.
The course you attend as part of the prize is also an amazing opportunity, giving you hands-on experience with advanced techniques, exposure to the latest materials, and the chance to meet inspiring people from across the profession. I would recommend the Award to any therapist who wants to develop their skills, build confidence, and be part of something that celebrates achievement and encourages growth within the profession.
KA: To any Foundation Trainees considering entering, I would say it’s a no-brainer. As part of foundation training, we’re required to present a complex case, which could likely involve anterior composite restorations – perfect for submission. Beyond showcasing your work, winning gives you the incredible opportunity to attend a world-class course in Belgium, expand your skills, and meet like-minded dental professionals who have also succeeded in the competition. It’s a chance to learn, network, and be inspired, all while gaining recognition for work you’re already doing as part of your foundation training.

You may be interested in our blog by Dr Juan Salmerón Ramírez, in which he reflects on entering a successful case in the inaugural Award.